
By Beatrice Nakibuuka
For years, 27-year-old Sarah Nakanwagi believed something was deeply wrong with her body. Her menstrual periods could disappear for months. She battled stubborn acne long after her teenage years had passed. No matter how carefully she tried to eat, the weight around her abdomen kept increasing. When she finally got married and struggled to conceive, relatives whispered painful suggestions about curses and infertility.
“I kept moving from clinic to clinic looking for answers,” she says and adds: “Some doctors said I was just stressed, while others told me to lose weight. But nobody explained why my body was behaving this way.”
Nakanwagi’s experience reflects the hidden reality of thousands of women living with a condition that has long been misunderstood. For decades, doctors referred to it as Polycystic Ovarian Syndrome, commonly known as PCOS. However, the condition has now officially been renamed Polyendocrine Metabolic Ovarian Syndrome, or PMOS, in a major global medical shift aimed at better explaining what women are actually experiencing.
The new name may sound technical, but specialists say it could change the lives of many women who have spent years suffering in silence.
Beyond “cysts” on the ovaries
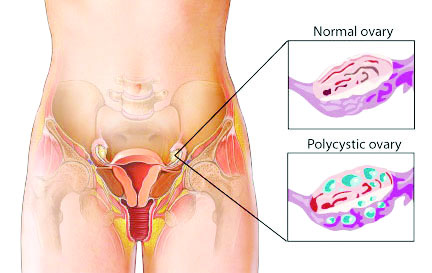
According to Dr Stephen Sematimba, a gynaecologist at Crystal Medical Centre, the previous name created widespread confusion because many people believed ovarian cysts were the defining feature of the condition.
“Many women would come with irregular periods, excessive weight gain, infertility, or abnormal hair growth, but when the ultrasound scan appeared normal, they were told they did not have the condition. Yet PMOS is much broader than what appears on the ovaries,” he explains.
He says the old term caused both patients and some health workers to focus too heavily on ultrasound findings while ignoring the hormonal and metabolic disturbances taking place inside the body.
Under the new understanding, doctors are now paying closer attention to how hormones, metabolism, insulin resistance, and reproductive health interact together.
Dr Joel Lwasa a gynaecologist at Kawempe Regional Referral Hospital says the renaming is important because it reflects the true nature of the disease.
“This is not just a fertility problem. It is a metabolic and hormonal condition that affects many systems in the body. A woman can have normal ovaries on scan but still suffer from PMOS,” he says.
The condition affects how the ovaries function, disrupts hormone balance, and interferes with the body’s ability to properly use insulin, the hormone that regulates blood sugar.
The symptoms women ignore
One of the greatest challenges surrounding PMOS in Uganda is that many women normalise the symptoms or fail to connect them.
Some women experience menstrual periods only a few times a year. Others develop severe acne, unwanted facial hair, thinning scalp hair, or rapid weight gain, especially around the abdomen. Many struggle with infertility without understanding the underlying cause.
Dr Sematimba says irregular menstruation is often one of the earliest warning signs.
“A normal menstrual cycle should generally come monthly. When someone repeatedly misses periods or goes several months without menstruation, it should not be ignored,” he says.
However, in many Ugandan communities, conversations about menstrual health remain uncomfortable. Young girls who experience abnormal cycles may fear discussing them openly with parents or guardians.
For married women, infertility often becomes the most painful consequence.
“In our setting, society places enormous pressure on women to produce children. When conception delays, the blame is usually directed at the woman, yet many times there is an underlying medical explanation like PMOS,” Dr Lwasa says.
A growing urban health problem
Doctors say PMOS is becoming increasingly common, especially in urban areas where lifestyle patterns have changed dramatically.
Uganda’s growing dependence on processed foods, sugary drinks, white bread, chapatis, fried snacks, and sedentary lifestyles is contributing to rising rates of obesity and insulin resistance.
Dr Sematimba explains that insulin resistance sits at the center of the condition for many patients.
“The body produces insulin but cannot use it efficiently. As a result, insulin levels rise and this triggers hormonal imbalance, including increased male hormones,” he says.
These elevated hormones contribute to acne, excessive facial hair, irregular ovulation, and fertility difficulties.
Women with PMOS also face a higher risk of developing Type 2 diabetes, high blood pressure, heart disease, and even endometrial cancer later in life if the condition is left unmanaged.
Dr Kwasa says: “This is why the new name emphasizes metabolism. We want women to understand that this condition goes far beyond the reproductive organs.”
Why diagnosis takes so long
Many women spend years searching for answers before finally receiving the correct diagnosis.
Part of the problem lies in limited awareness. Some women assume their symptoms are simply part of normal womanhood. Others first seek help from herbalists or unqualified clinics.
Cost is another major barrier. In private facilities around Kampala, consultation fees with a gynecologist can range between Shs50,000 and Shs150,000. Hormonal blood tests may cost over Shs200,000, while repeated ultrasound scans further increase expenses.
Although public hospitals such as Mulago National Referral Hospital and Kawempe National Referral Hospital offer gynecological services, patients often face long queues and delayed appointments. Some women become frustrated and abandon treatment midway.
“PMOS is not something managed in one week or one month,” It requires long-term follow-up and lifestyle adjustment,” Dr Lwasa says.
The condition is usually diagnosed through a combination of symptoms, menstrual history, hormonal tests, physical examination, and sometimes ultrasound findings.
The dangerous rise of fake remedies
As awareness of hormonal disorders grows, social media has become flooded with herbal mixtures and unverified “fertility boosters” claiming to cure hormonal imbalance instantly.
Doctors warn that many desperate women spend huge sums of money on treatments with no scientific backing.
“We have patients who come after taking multiple herbal products that worsen their weight, damage the liver, or delay proper treatment,” says Dr Sematimba.
He advises women to seek care from qualified gynecologists, endocrinologists, or licensed medical facilities rather than relying entirely on online advice.
“There is no miracle drink that cures PMOS overnight,” he says and adds that management requires proper medical evaluation.
A new approach to treatment
Unlike in the past, when treatment focused mainly on inducing menstruation or helping women conceive quickly, doctors are now adopting a broader long-term management strategy.
Lifestyle modification remains one of the most important interventions.
Dr Lwasa says even modest weight loss can significantly improve hormonal balance and ovulation.
“We encourage women to become physically active through walking, jogging, home exercises, or even regular domestic work and gardening,” he explains.
Nutrition also plays a major role. Specialists now encourage women to reduce highly refined carbohydrates and excessive sugar intake while increasing fibre-rich local foods.
Traditional Ugandan foods such as millet, beans, sweet potatoes, green vegetables, and matooke are increasingly being recommended over highly processed diets.
Dr Sematimba notes that many women mistakenly believe starvation is the solution.
He says: “We do not tell patients to stop eating. We teach them how to eat better and more sustainably.”
Medication may also be prescribed depending on symptoms. One commonly used drug is metformin, which helps improve insulin sensitivity and regulate blood sugar levels.
For women hoping to conceive, fertility treatment may be introduced once hormonal balance improves.
“The good news is that many women with PMOS can still become pregnant with proper treatment and lifestyle adjustment,” Dr Lwasa says.
Young girls are also at risk
Specialists are increasingly concerned about rising hormonal disorders among adolescents.
Teenage girls who begin experiencing extremely irregular periods, severe acne, or rapid unexplained weight gain should not automatically dismiss these changes as normal puberty.
Early diagnosis can prevent years of complications later in life.
Dr Sematimba says parents need to create safe environments where girls can discuss menstrual health openly.
“In many homes, menstruation is still treated as a secret topic,” he says. That silence delays medical attention,” he says.
He also warns against body-shaming young girls who gain weight because some may already be struggling with hormonal imbalance.
Breaking the silence
For many women, the biggest relief comes not from medication alone but from finally understanding what has been happening to their bodies.
After years of confusion, Nakanwagi says finally receiving a diagnosis changed her outlook completely.
“I stopped blaming myself. I realised I was dealing with a medical condition, not a curse.”
Today, she is undergoing treatment, exercising regularly, and learning how to manage her symptoms.
Doctors believe the renaming from PCOS to PMOS marks an important turning point in women’s healthcare because it pushes both patients and health workers to look beyond the ovaries and address the broader hormonal and metabolic crisis affecting women’s lives.
Dr Lwasa says, “This condition is manageable. The earlier women seek help, the better the outcomes.”
Dr Sematimba agrees, adding that awareness remains the strongest weapon.
“Women should pay attention to their bodies. Irregular periods, unexplained weight gain, acne, or difficulty conceiving should never be ignored,” he says.


